 Reserve with Google
Reserve with Google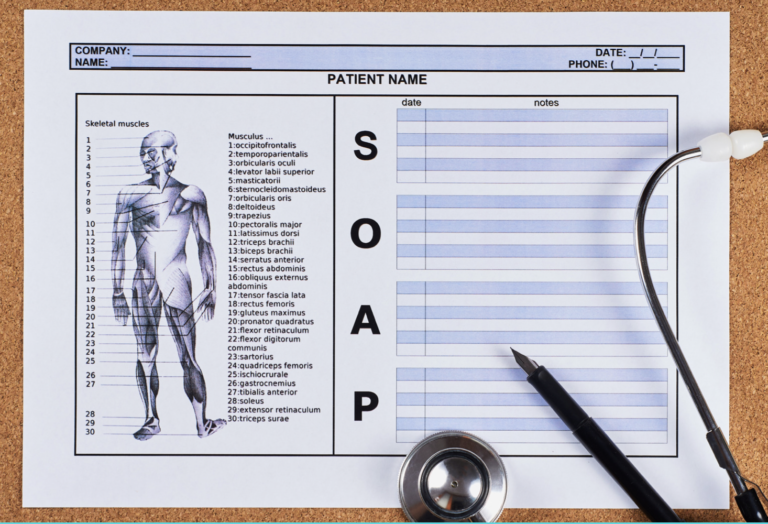
For centuries, massage and physical therapy have been practiced to relieve people of disabilities and illnesses. Yet, providing and documenting the utmost patient care has never been as streamlined as it is today with electronic medical records.
An EMR software offers sophisticated tools including electronic medical charting and SOAP notes. These resources have evolved into a popular communication tool between interdisciplinary healthcare professionals.
A therapy appointment software or medspa practice management software provides healthcare practitioners with niche type resources which help you (and your clinical staff) deliver better patient care.
Let us delve in and peruse how an EMR system can actually improve quality of healthcare.
Collaborative Practice Management Software
Do rapidly changing demands, information overload, cumbersome documentation, and administrative tasks become overwhelming? If you want real-time clinical and business intelligence, a HIPAA compliant practice management software is necessary for your healthcare clinic.
How can a practice management software save you time and money? During our preliminary research, we interviewed a handful of physical healthcare practitioners that transitioned from the “pen and paper method” to an electronic method of patient care in the past year. Here is a synopsis of their overall experience:
- 45% less time spent on documentation
- 25% more detailed clinical content captured
- 1 hour per day saved on documentation
Our hypothesis has always accounted for the importance of electronic resources in documenting patients’ progress and better patient care, but we were ecstatic to learn the time and energy it really saved practitioners. A practice management software provides smooth connections with patients through the integrated portal, which includes:
- Online scheduling
- Video appointments and teletherapy
- Helping practitioners more effectively diagnose patients, reduce medical errors, and provide safer care
A big component of a practice management software is electronic medical records (EMR). Let’s consider the real advantages of transformed health care.
Can Electronic Medical Records Improve Quality of Healthcare?
The results are in and yes, electronic medical records can improve quality of care. Some components that contribute to this include:
- Streamlined workflow
- Monitor patient flow from the virtual waiting room to triage to physical health visits
- Reduction of manual paperwork which helps to reduce cost
- Communication & better record keeping
- Precision in clinical care and enhanced communication with healthcare specialists
- Enabling quick access to patient records for more coordinated, efficient care
- Involving patients in their health by sharing results faster, electronically and securely
- Accurate, up-to-date, and complete health records
- Enhanced care
- Provides healthcare providers with more precise diagnosis and reduces medical errors to improve safety and health
- Compliance
- Helping promote legal documentation and records in terms of liabilities
If you encounter a case which requires critical care, say a rehabilitation injury or a patient with a disability, it is critical for current and future healthcare providers and therapists to access the patient’s full H&P (history and physical examination).
For instance, if a patient is starting physiotherapy and has a pacemaker, the therapeutic plan needs to be based on the patient’s debility, as documented by their cardiologist. Since certain electronics and stimulators need to be avoided on a patient with an implanted device, access to proper documentation becomes as crucial as life and death.
With a comprehensive EMR system that allows patient management beyond just records, “Alerts” can be set up to notify the practitioners of a patient’s particular details related to their health:

Every single detail of your patient, including symptoms, allergies, treatment records, SOAP notes, and anatomy charts are stored securely and digitally with cloud based access from anywhere, anytime.
Electronic Medical Forms
Schedule and share electronic forms, questionnaires, or consent forms via email or waiting room kiosk mode. To save up to 15 minutes per appointment, digitally send intake forms to your patient and receive them manually, securely stored in the patient’s file for easy access. This feature is imperative when it comes to fast transfer of patient records to say laboratories, certified sports specialists, or medical imaging facilities.
Below is an example of an electronic form template. The healthcare professional can upload an anatomy photo(s) to be used to annotate areas of treatment, modify notes, track revisions and document comprehensive healing progress:

If you are too busy to type it, draw it; Use visual markers on anatomy charts to enhance precision in your patient care strategies. A picture can speak a thousand words!
There are other benefits to using the (right) EMR tool. For instance, if you’ve saved a patient’s details in the “Patient Detail” section of their profile, your patient no longer needs to fulfill their preliminary details when fulfilling electronic forms. In other words, when your patient is fulfilling a form that you require of them, their preliminary information will be automatically populated with the right EMR tool.
Charting Made Easy with Digital Anatomical Drawings
Electronic charting becomes particularly useful when a healthcare professional, say a physiotherapist, encodes visualizations in detail and needs to explain the interpretations to other therapists via digital technology. From a cognitive perspective, using annotations for additional diagnosis expands learning and precision in physical care. Annotations include highlighting, pining, naming, labeling, and commenting aspects of visual representations.
Other benefits of electronic charting include:
- Less paperwork and improved patient and physical documentation
- Zero storage space required
- No additional secure guard for papers in case of theft or fire
- Imagine this; 500 sheet of paper weighs 5 pounds and costs storage money
- An ethical and paperless practice which 88% of customers demand.
- Fast access to patient records, even if you work at multi-location clinics
- Mobile and remote access to records
The Importance of SOAP Notes
SOAP notes were developed by Dr. Lawrence Weed in the 1960’s at the University of Vermont as part of the “problem-oriented medical record.”
To keep communication flowing seamlessly between providers inter alia safeguard healthcare providers from liability, detailed patient notes are compulsory. To freshen your memory, let’s review what SOAP notes consist of:
S = Subjective: This is the information that a therapist collects from their patient. For instance, “When I sleep on my side, my shoulders are in excruciating pain” is a subjective comment without the therapist’s perception. Note: Providers should not include their own analysis in the subjective.
O = Objective: In this section, any exercise and treatments executed should be documented. For instance 1) Exhibited proper positioning for sleeping with low constraints on shoulders 2) Exercised shoulder flexion muscles including the anterior deltoid, pectoralis major and coracobrachialis. 3) Shear wave ultrasound 1. 5 w/cm2 for (two) 10 minute sessions focusing around anterior deltoid muscle. Note: Think of it this way: If a patient’s pain escalates, the objective must be clear to understand by other specialists, or even an orthopedist.
A= Analysis/Assessment: In this section, the healthcare provider can write their own diagnosis, such as “Patient is experiencing pain in the shoulder joint, stiffness and reduced range of motion– indications are pointing to arthritis of the shoulder.” This feedback becomes highly valuable, particularly if your patient has been in an accident and the case manager can look for functional diagnosis. Note: The more precise the analysis, the better the therapeutic plan can be customized.
P = Plan: Here is where the healthcare provider documents progress and a therapeutic plan, such as “For a temporary relief, a cortisone injection was given to ease the pain and inflammation. The patient’s pain has reduced by 40%.”
When using SOAP notes, it is important to write a clear note in the record that indicates the thought process supporting the alternative treatment you have designed for your patients.
Are SOAP Notes Legal Documents?
Soap notes are not required by law but some healthcare associations require therapists to maintain their client soap notes for at least 11 years. Why? Because proper patient documentation via SOAP notes is an excellent resource to protect healthcare professionals against liabilities, if any arise. A soap note is then a legal document that can be used as the formal, complete record of encounters.
In other words, yes SOAP notes provide well grounded, structured documentation in avoiding legal lawsuits.
Read more: Med spa laws by US states
EMR Does Improve Quality of Care
When it comes to patient care, electronic medical records can improve the quality of healthcare. With data driven tools like electronic charting and SOAP notes, healthcare practitioners can document and provide enhanced patient after care. Most importantly, an EMR improves communication flow and interactions among primary care providers, patients, and other healthcare practitioners.
In addition, having structured data digitally allows for better reporting and insights into daily work of the practitioners. If you are looking to improve quality of care and streamline an EMR software with your clinic’s processes, book a demo with Yocale today.
